Plan Of Care For Jim And His Family
Question:
Answer:
Introduction
The present report is on an 89 year old male patient Jim Karas who had been transferred from the emergency department to Intensive Care Unit (ICU) after he suffered hypertensive condition and was not breathing spontaneously. Accordingly, 3 lumens central venous access device as inserted to provide intervention. The aim was to relief him from the hypotensive condition after administration of IV fluid. After a hospitalisation period of one week, on day 8 he was taken off inotropes. He was found to be in physically and mentally stable condition while being transferred to medical ward. After being stable in the medical ward, he is now ready to be discharged.
Plan of discharge
A well-planned discharge summary has a crucial role in improvement of the health condition of the patient and the overall wellbeing. This is done to reduce the risk of harm and minimise the rate of readmission, thereby facilitating a positive experience for the patient (Zaccagnini and White 2015). Share transfer of care for NSW core principles are to be utilised for planning the discharge of Jim. The stepwise process of discharge would be as follows-
- Admission- Transfer of care planning together with transfer of care Risk assessment are crucial to be made within the first 24 hours of patient arrival. The multidisciplinary team is to make the plan of care.
- Multidisciplinary team meeting- At the time of multidisciplinary team meeting, there should be an effective communication between Jim and his family members, and the team members. The team must communicate to the individuals about the care that is proposed to be given to the client.
- Estimated date of discharge- Estimated date of discharge is to be articulated within 24 hours of admission of Jim. This date is to be informed to Jim and his family members, and the multidisciplinary team. Any possible delay is also to be communicated accordingly.
- Referrals- Referrals are crucial to be made long before the date of discharge in order to ensure that the care planning is managed in an effective manner. A need assessment is to be done for Aged Care Assessment Team (ACAT) for inclusion in the community page.
- Transfer to home- A checklist is to be followed while transferring Jim back home. This includes medication review by pharmacist, discharge summary, patient education about medication. The community nurse and GP must discuss the means of transferring Jim to home with Angela.
The need of a well-documented discharge summary is crucial for Jim and Angela for ensuring that the care needs of the patient are met in a comprehensive manner. The aim would be to enhance the quality of life of the patient while his stay at home. As Jim is residing in his home, his wife Angela would serve as the primary care giver. It is to be noted that Amara has been diagnosed with COPD and depression. It is therefore the discharging nurse’s responsibility to communicate with the community service provider for ensuring that the share transfer of care is handed over in an accurate manner. As Jim resides in Randwick council, care referral is to be made to the services, which are available nearby. In addition, they are to be affordable.
ST Basil home Randwick is therefore the ideal service where the transfer of care can be handed over in accordance to the best interest of the patient. A number of services are provided by ST Basil Home that are appropriate for the client in the present case. These include the following-
- Carers are available who can support the couple with their activities of daily living (ADLS) like cleaning and washing.
- Community nurses are available who can help with regular dressing on the wound site and guide with medication management for both Jim and Amara.
- Transport services can be availed that are important for medical appointment and social activities.
- Provision for interpreter service is present with which Amara can communicate and express her feelings.
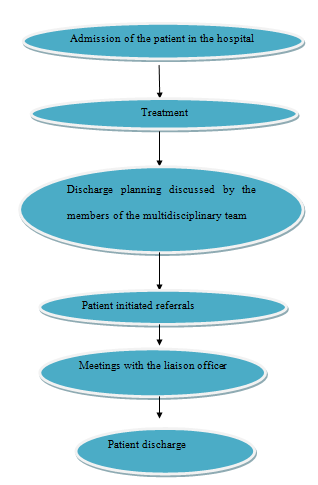
Discharge protocol (Source: created by author)
Legal and ethical principles of decision making
As per the case study, Angela considered placing Jim and Amara in residential care due to personal constraints. The aim was to ensure appropriate care and continuous surveillance for her parents to promote health and wellbeing for her parents. Patient education is required after placing them in the residential care. Consideration is to be given to the preferences of the family members while educating the clients (Reinhard et al. 2012).
There are four major principles of strength based nursing and health care, that is provision of family centred care, empowerment, promotion of health and healing and collaborative partnership (Butts and Rich 2012). Jim required a family centred care; hence it is not very sure that any residential care would be suitable for him. St. Basil’s home can be opted as it can provide home based support which would help to empower the patient. Older persons already suffer from emotional turmoil hence a proper home care support and a collaborative care by the caregivers, family, GPs and other community support can have a healing effect on the health.
Collaborative partnership is considered one of the important factors of strength based nursing. The family members and the home support should explain each and every proceeding at every opportunity and should reassure the patient (Barry and Edgman-Levitan 2012).
The four principles of nursing ethics are autonomy, beneficence, non- maleficience and Justice (Oliveira et al 2012). It can be seen from the case study that Angela was keen at providing some additional support for their parents. Jim might not show interest in taking any additional help and want to take care of his wife alone. However, the health status of both Jim and Amara requires a constant physical as well as mental support. Considering the legal side, it is not wrong to prefer physical well being over emotional well being; hence Jim and Amara could be kept under residential care. But considering the nursing codes of ethics patients have the right to make decisions about their medical care without the health care provider trying to influence the decision (Barry and Edgman-Levitan 2012). Patient autonomy does prefer to educate the patient about the type of care that they can adopt but does not allow anyone to force the patient to take any decisions. Hence, when Jim does not want to go to any aged care facility it is necessary to respect their decision and think of some alternatives. There are several community nursing facilities that provide home support or set up routine check up regimen as and when required (Harkness and DeMarco 2016). Certain organisation in community are specialised in health assessment and collaborative care and support planning to patients (Butts and Rich 2012). Such a proactive approach can be helpful both in maintaining the autonomy and the dignity in patient as well as look after their physical well being (Harkness and DeMarco 2016). A collaborative care of approach is required as Amara needed care for her COPD and Jim needed an overall support for his health. As already mentioned that Jim lived in Randwick, the Randwick community service provides a lot of services. The Randwick community council provides attractive home care packages for elderly people. There are suitable ambulatory care services for the emergency patients.
Autonomy to a patient refers to the right of the patient to refuse, accept or terminate any treatment under any coercion, influence or prejudice. Ethical dilemmas may arise while balancing the autonomy to Jim and his wife’s safety and well being. For most of the older people autonomy is extremely important for the good quality of life as well as well s being able to live independently in their own home unless restricted by very poor health status. Elderly people when institutionalised often face with ill behaviour from the other residents or the caregivers which can destroy their dignity and integrity. Even when institutionalised they should be involved in the decision making process. Lindberg et al.(2014) has stated that the perception of autonomy and justice allows people living with depression and anxiety to design their lives in accordance with their personality and values.
Provision of culturally safe care
Cultural safety may be defined as an environment that provides socially, spiritually, physically and emotionally safe care to a person. It is necessary for a caregiver to remain aware of the culture differences and similarities of the culture of the patient. One of the main ethics of nursing is accept any culture without judging them (Harkness and DeMarco 2016). Residing in a residential aged care may be demeaning for Jim’s culture hence the clinical professionals should look forward to arrange for a home care support instead of sending them to a residential care. Jim or Amara might not want to receive care from an opposite sex person. Again Jim or Amara might not want a caregiver form of a home support coming from a different culture as they might think that, the caregiver will not be able to address their needs owing to the different culture. In such cases cultural safety can be accomplished by providing them home support as per their choices
Conclusion
The case study provides us with the information that Jim had recently been discharged from a hospital after been treated for hypoxia and hypotension due to his exposure to carbon monoxide. Jim suffered from CVAD related blood stream infection which was being treated before his discharge. Although Jim doesn’t want to receive any additional help for their care yet their daughter and the health care professional suggest them to opt for additional support. In context to this, it is advisable to adopt a home care support that would help manage Amara and Jim’s health as well as their daily activities. Antibiotics should be continued for preventing further infections.
References
Barry, M.J. and Edgman-Levitan, S., 2012. Shared decision making—the pinnacle of patient-centered care. New England Journal of Medicine, 366(9), pp.780-781.
Butts, J.B. and Rich, K.L., 2012. Nursing ethics. Jones & Bartlett Publishers.
Ford, A.H. and Almeida, O.P., 2015. Pharmacological interventions for preventing delirium in the elderly. Maturitas, 81(2), pp.287-292.
Harkness, G.A. and DeMarco, R.F., 2016. Community and public health nursing: Evidence for practice. Wolters Kluwer.
Inouye, S.K., Westendorp, R.G. and Saczynski, J.S., 2014. Delirium in elderly people. The Lancet, 383(9920), pp.911-922.
Lindberg, C., Fagerström, C., Sivberg, B. and Willman, A., 2014. Concept analysis: patient autonomy in a caring context. Journal of advanced nursing, 70(10), pp.2208-2221.
Oliveira, V.C., Refshauge, K.M., Ferreira, M.L., Pinto, R.Z., Beckenkamp, P.R., Negrao Filho, R.F. and Ferreira, P.H., 2012. Communication that values patient autonomy is associated with satisfaction with care: a systematic review. Journal of Physiotherapy, 58(4), pp.215-229.
Reinhard, S.C., Levine, C. and Samis, S., 2012. Home alone: Family caregivers providing complex chronic care. Washington, DC: AARP Public Policy Institute.
Szebehely, M. and Trydegård, G.B., 2012. Home care for older people in Sweden: a universal model in transition. Health & social care in the community, 20(3), pp.300-309.
Zaccagnini, M. and White, K., 2015. The doctor of nursing practice essentials. Jones & Bartlett Learnin
Use the following coupon code :
SAVE10